
DHT hair loss starts long before you notice it.
By the time most people are searching for answers, the thinning has been going on for a year or two already. The hairline has quietly moved back. The crown looks a little more exposed in photos. The hairs coming out in the shower are thinner than they used to be.
And then comes the search. Which usually leads to a wall of product ads, contradictory advice, and zero actual explanation of what is happening inside your scalp.
So let’s start there. What DHT is, what it does to your follicles, and what you can realistically do about it. No scare tactics. No miracle promises.
If you want to know where your hair loss actually stands right now, a medical scalp assessment at UniquEra gives you a clear picture before any decision is made.
DHT stands for dihydrotestosterone. Your body makes it by converting a portion of testosterone using an enzyme called 5-alpha reductase. This happens in several tissues including your scalp, skin, and prostate.
It is a natural hormone. Not a glitch, not a toxin. During puberty, DHT drives the development of male characteristics: body hair, facial hair, genital development. Your body needs it at that stage.
The problem shows up later. In adulthood, some scalp follicles are genetically wired to overreact when DHT binds to them. That reaction, repeated across years and dozens of growth cycles, is what drives dht and hair loss.
DHT is doing exactly what it is designed to do. The problem is the follicle’s response to it.

Most people assume hair loss happens because DHT destroys follicles. It does not. The follicle is still there. What DHT does is quieter than that, and slower.
It shrinks them.
Not overnight. Not in one dramatic event. Over years, across dozens of growth cycles, DHT gradually makes certain scalp follicles smaller and less capable of producing the kind of hair you can actually see.
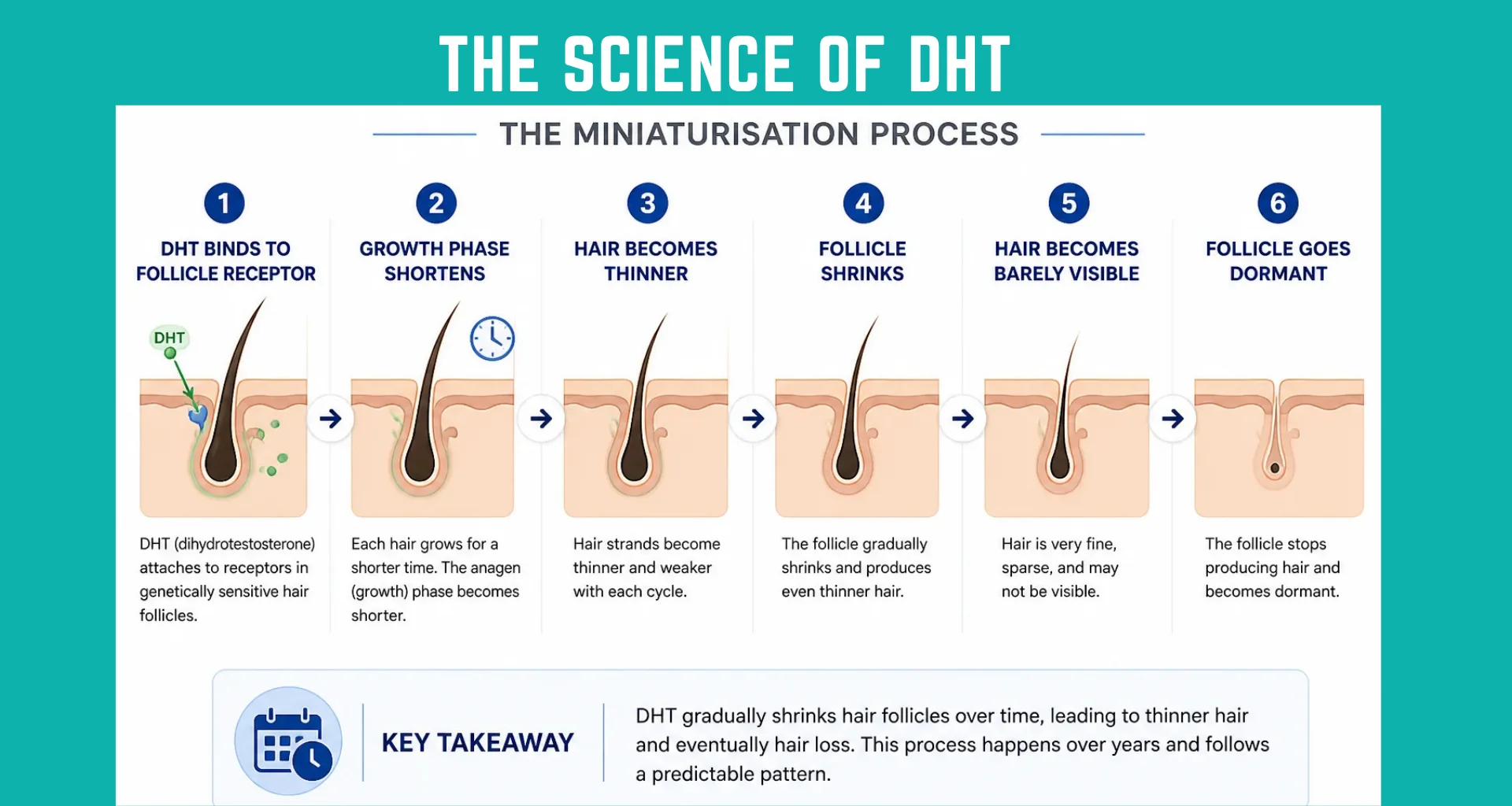
This process has a name: miniaturization. And understanding it changes how you think about every treatment option.
Your scalp follicles have androgen receptors on them. Think of these as binding sites. DHT attaches to them. In follicles that are not sensitive to DHT, nothing much happens. In follicles that are genetically sensitive, that binding triggers a biological reaction that disrupts the normal hair growth cycle.
Three things happen as a result, each one building on the last.
The growth phase gets shorter. Healthy hair spends years in the active growth phase, called anagen. A single hair can grow for three to seven years before it sheds. DHT shortens this phase significantly in sensitive follicles. Hair spends less time growing and more time in the resting and shedding phase, called telogen. The result is hair that never gets the chance to grow long or thick before it falls out.
The follicle shrinks with each cycle. Every time a miniaturizing follicle goes through a growth cycle, it produces a slightly thinner and shorter hair than the one before. This is not dramatic from cycle to cycle. Across ten or twenty cycles though, the difference is visible. What was once a thick strand becomes a thin one. What was once a long hair becomes short.
Thick hair turns into fine, invisible hair. Healthy scalp hair is called terminal hair. It is thick, pigmented, and visible. As miniaturization progresses, the follicle stops producing terminal hair and starts producing vellus hair instead. Vellus hair is the fine, colorless, almost invisible hair you see on a child’s cheek. The follicle is technically still alive. It is just no longer producing anything you can see.
In the final stages, the follicle can stop producing any visible hair at all. Once that happens, getting it working again without surgical intervention is very unlikely.
The whole process can take anywhere from a few years to a few decades depending on genetics. That slow pace is part of why it catches people off guard. There is no single moment when it starts. It has usually been happening quietly for years before the mirror makes it obvious.

Androgenetic alopecia is the clinical name for pattern hair loss. It is the most common form of hair loss in both men and women.
The name is more descriptive than it sounds:
• Andro refers to androgens, the hormone group that includes DHT and testosterone
• Genetic refers to the inherited sensitivity that determines how your follicles respond
• Alopecia means hair loss
It is not a disease. It is a genetic trait that determines how your follicles react to a hormone that is already naturally in your body. You are not producing too much DHT. Your follicles are just more reactive to the amount you have.
This matters when thinking about treatment. You are not fixing a hormonal disorder. You are managing how genetically sensitive follicles interact with a normal hormone.

DHT is the primary hormonal driver of androgenetic alopecia causes — to understand how it differs from testosterone, read our guide on DHT vs testosterone. But genetics decide how severe the reaction actually is.
Here is what most people get wrong: it is not how much DHT you have that determines whether you lose hair. It is how sensitive your follicles are to it.
Two men can have identical DHT levels in their blood. One goes bald at 28. The other still has a full head of hair at 65. The difference is in the androgen receptor gene, called the AR gene. Variations in this gene make some follicles overreact even to normal DHT levels.
Another common myth: this gene only comes from your mother’s side. That is not accurate. The AR gene sits on the X chromosome, which comes from your mother. But other genes that contribute to pattern hair loss sit on different chromosomes and can come from either parent. Your father’s hairline is relevant. So is your paternal grandfather’s.
Genetics set the rules. They do not write a guaranteed outcome. But knowing your family history gives you useful information.
DHT hair loss is not a male-only issue. Women produce DHT too, in smaller amounts. And in women who are genetically sensitive, the same miniaturization process happens. The difference is in the pattern.
| Factor | Men | Women |
| Primary pattern | Receding hairline, crown thinning | Diffuse thinning across top of scalp |
| Frontal hairline | Usually recedes | Usually preserved |
| Progression scale | Norwood Scale (7 stages) | Ludwig Scale (3 stages) |
| DHT levels | Higher overall | Lower, but follicles can still be sensitive |
| Age of onset | Often late teens to mid-20s | Often post-menopause, but can be earlier |
| Treatment options | Finasteride, minoxidil, transplant | Minoxidil primarily, transplant in suitable cases |
In women, estrogen partially offsets the effects of androgens during reproductive years. After menopause, estrogen drops and DHT’s relative impact increases. That is why many women notice thinning starting in their 40s and 50s.
The biology behind DHT and hair loss is the same in both sexes. The pattern and hormonal context differ.
If DHT were the only factor, hair loss would happen evenly across the whole scalp. It does not, and the reason is straightforward.
The follicles at the crown and temples have a much higher density of androgen receptors than the follicles at the back and sides. More receptors means a stronger reaction to DHT. These areas are genetically more vulnerable, and they show it first.
The follicles at the back and sides have far fewer androgen receptors. They are largely DHT-resistant. Even in men who have been losing hair for decades, these follicles keep producing healthy hair.
This is not random variation. It is genetics determining which follicles are vulnerable and which are not.
That ring of resistant hair around the sides and back is not just a cosmetic feature. It is the biological foundation that makes hair transplant surgery a logical solution for DHT hair loss. More on that shortly.
Not all hair loss has the same cause. Thyroid problems, low iron, stress, and autoimmune conditions can all cause shedding. Getting the cause right matters before deciding on any treatment path.
Signs that point toward dht and hair loss:
• The loss follows a pattern, not sudden or uniform shedding across the whole scalp.
• Crown thinning or a receding hairline in men, or widening part line in women.
• Gradual change over months and years, not a sudden shed event.
• Family history of pattern hair loss on either parent’s side.
• Hair in thinning areas is getting shorter and finer over time.
• Thyroid, iron, and other health markers are normal.
A blood test for DHT levels is often not the most useful diagnostic tool. Your bloodstream DHT level does not tell you how sensitive your follicles are to it. A clinical scalp exam, combined with trichoscopy (scalp examination under magnification), shows far more.
Trichoscopy can catch miniaturized follicles early, before the pattern is visible to the naked eye. That matters because the treatment window is wider when follicles are still active but shrinking.
Whether can dht damage be reversed depends on how far the miniaturization has gone. The honest answer sits somewhere between yes and no, depending on your stage.
What can be done: Active miniaturization can be slowed or paused. In follicles that are shrinking but still producing some hair, partial recovery is possible with proven treatments. This is what clinical evidence supports for early-to-moderate loss.
What is not reliably possible: Follicles that have been dormant for a long time do not respond predictably to non-surgical treatment. A follicle that stopped producing visible hair years ago is a very different target from one still producing thin hair.
Why the timing matters: Acting while follicles are still miniaturizing but active gives treatment the best shot. Waiting until large areas are fully bald shifts the options almost entirely toward surgical restoration. This is not about pressure. It is just how the biology works.
No single treatment fits every situation. What makes sense depends on your age, how far the loss has progressed, your goals, and your overall health. Here is an honest breakdown.
| Treatment | What It Does | Best For | Key Limitation |
| Finasteride | Blocks 5-alpha reductase, reduces DHT conversion | Men with active early-to-moderate loss | Requires ongoing use. Effects reverse if stopped. |
| Minoxidil | Improves blood flow to follicles, extends growth phase | Supporting existing hair, early thinning | Does not target DHT. Needs continuous use. |
| PRP | Growth factors from your blood support follicle health | Early thinning, post-transplant support | Results vary. Not standalone for significant loss. |
| Hair Transplant | Moves DHT-resistant follicles to thinning or bald areas | Stable loss with sufficient donor supply | Requires planning. Does not stop loss in untreated areas. |
| DHT-blocking shampoos | Reduce DHT at the scalp surface | Mild early-stage support only | Limited clinical evidence for reversal. |
These options are not mutually exclusive. Using finasteride to slow active loss while a transplant addresses already-lost areas is a common and sensible combination. The right mix is a clinical decision, not something a comparison table can determine on its own.
A medical assessment at UniquEra maps your follicle health, looks at your donor area, and gives you an honest picture of your options before anything is decided.
Look at almost anyone with male pattern baldness. The top is thinning or gone. The back and sides still have hair. Even in men who have been losing hair for thirty years.
That is not a coincidence and it is not random. Those follicles are built differently at a biological level.
They have far fewer androgen receptors than the follicles at the crown and temples. So when DHT arrives, they barely react. They do not miniaturize. They keep growing thick, healthy hair year after year, even while the top of the scalp changes.
A simple way to think about it: two people working in the same stressful environment. One shuts down under pressure. The other stays steady no matter what. Same conditions, completely different response. That is what is happening between your follicles. Same DHT, same scalp, completely different reaction. Because the follicles themselves are genetically different from each other.
This is not just interesting. It is the entire reason hair transplant surgery works.

A hair transplant for androgenetic alopecia works because of a biological principle called donor dominance.
When DHT-resistant follicles from the back and sides are moved to an area where hair has been lost, they do not change. They do not pick up the behavior of their new location. They keep doing what they were doing before. They grow. They stay thick. They do not miniaturize.
The transplanted hair does not know it has moved. It only knows what it is built to do. And what it is built to do is resist DHT.
This is why a well-planned hair transplant for male pattern baldness holds up over years, in a way that topical or oral treatments alone cannot replicate for areas that are already bald.
Because the follicles used in the transplant are DHT-resistant. That is the short answer.
Most hair loss treatments manage DHT activity. Finasteride reduces how much DHT your body produces. Minoxidil supports struggling follicles. Both require ongoing use because they are managing a process, not replacing what has been lost.
A hair transplant does something different. It replaces the lost follicles with ones that are biologically built to survive DHT. The follicles taken from the back and sides of your scalp have never miniaturized. They have lived alongside DHT your whole life and kept producing healthy hair regardless. When moved to a bald area, they continue doing exactly that.
They do not need DHT blockers to survive in their new location. They already are resistant.
No, not from DHT. The transplanted follicles came from a DHT-resistant zone and they keep that resistance permanently after the procedure.
What can happen is different: the native hair around the transplanted area, hair that was not part of the transplant, can keep thinning if DHT activity is not being managed. That is not the transplant failing. It is the underlying condition continuing in the surrounding follicles that were always vulnerable.
This is why medical management after a transplant matters. The transplanted hair holds. The surrounding hair needs ongoing support.
For the transplanted areas, yes. For the broader condition, it is one part of a complete plan.
| What the Transplant Does | What It Does Not Do |
| Restores hair in areas where follicles are gone | Stop DHT from affecting surrounding non-transplanted follicles |
| Uses follicles that are permanently DHT-resistant | Replace the need for medical management of ongoing loss |
| Produces results that hold up long term in treated areas | Guarantee surrounding native hair stays thick without support |
A transplant is not a cure for androgenetic alopecia. It restores specific areas permanently, and works best when paired with a plan to manage what continues around it.
Not everyone is ready for a transplant right now. A clinic worth trusting will tell you that before recommending one.
| Assessment Factor | What It Means for You |
| Hair loss is stable | The pattern has not changed significantly in the last 12 months, or is being controlled with medication |
| Enough donor hair available | The back and sides have sufficient healthy, DHT-resistant follicles to cover the target area |
| Target areas have inactive follicles | Little to no active growth remains in those zones that could be preserved non-surgically |
| Age and pattern are predictable | The long-term direction of loss can be reasonably mapped so the result holds up over years |
A transplant planned without checking all four of these factors can look unnatural over time, or leave you with too little donor hair for future sessions.
A transplant done at the wrong time can create more problems than it solves.
| Situation | Why Waiting Makes Sense |
| Hair loss is still actively progressing | Transplanting into an area that keeps thinning around it can look patchy within a few years |
| Young patient with aggressive early loss | The full pattern is not yet clear. Planning a transplant now risks designing around an incomplete picture |
| Not enough donor hair for the area | Taking too many grafts today limits what is possible in future sessions |
| Active loss not medically managed | Transplanting without addressing ongoing DHT activity is like fixing one leak while others keep opening |
None of this rules out a transplant. It means the timing and plan need to be right for the result to actually hold.
It depends on your individual picture, not your age or how long you have been losing hair.
There are two windows in DHT hair loss.
Window 1: Preservation. Follicles are still active but miniaturizing. Non-surgical treatments like finasteride and minoxidil work best here. The goal is to slow the process and protect what remains. A transplant may not be the right step yet, but getting an evaluation at this stage gives you the most options going forward.
Window 2: Restoration. Areas have already been lost and follicles in those zones are no longer active. Non-surgical treatments cannot bring back what is gone. A diffuse thinning hair transplant is planned differently depending on whether the loss is in the hairline, mid-scalp, or crown.
Most people arrive somewhere between the two. That is why an assessment matters more than any general timeline.
The worst time to start thinking about this is when the loss is advanced and the donor supply is limited. Getting an evaluation early, even if surgery is not yet needed, tells you which window you are in and what your options look like now versus in five years.
UniquEra, recognised as the best hair transplant clinic in Istanbul, does one thing: hair restoration. No other procedures, no split focus.
The Medical Directors at UniquEra have over a decade of hands-on hair transplant experience, supervising each case personally. The team that assesses you is the team that plans your care throughout.
Patients who arrive having already decided they want DHI or FUE Sapphire based on online research are making a clinical judgment without clinical information.
At UniquEra, the technique is determined after a full assessment. FUE Sapphire is used for larger cases requiring higher graft counts. DHI Choi is used for precision work where minimizing skin trauma allows faster recovery. That decision belongs to the medical team, not the patient.
| Assessment Factor | Why It Matters |
| Hair loss stage and pattern | Determines scope and technique |
| How fast the loss is progressing | Affects timing and whether medical management is needed first |
| Donor area density and quality | Sets the ceiling on what is achievable |
| Long-term loss trajectory | Makes sure the plan holds up over years, not just this procedure |
| Graft count vs donor preservation | Protects options for future sessions if loss continues |
90% of new patients at UniquEra come through word-of-mouth referrals. That number comes from patients who had their own experience and told someone else about it.
A consultation here is a medical assessment. If a transplant is not the right step for you at this stage, that is what you will hear.
DHT hair loss follows a predictable biological path. A natural hormone, a genetic sensitivity, and a slow progressive reaction in specific follicles. The result is miniaturization, thinning, and eventually visible loss in a pattern your genetics set long before you noticed it.
That process is not entirely out of your control. Proven treatments can slow it. A well-planned hair transplant can address areas where DHT has already caused permanent loss, using follicles that carry their DHT resistance with them into their new location.
What matters most is an accurate picture of where you actually stand, and decisions made from that, not from product claims or forum threads.
If you want a clear, honest read on your hair loss and your real options, the team at UniquEra is available for a medical consultation. No pressure, no predetermined packages. Just an honest look at your scalp and a straight conversation about what makes sense for you.
No. The miniaturization process does not reverse without intervention. The earlier you act, the more options are available for preserving existing hair and recovering recently thinned follicles.
Pattern-based loss at the crown or temples in men, or diffuse thinning at the top in women, combined with a family history, points strongly to DHT. A clinical scalp assessment is more reliable than a blood test for confirming this.
DHT is dihydrotestosterone, an androgen your body makes from testosterone using the enzyme 5-alpha reductase. It is natural and necessary, but in genetically sensitive people it causes scalp follicles to shrink over time.
Without treatment, the miniaturization continues. With medical treatment, it can be slowed or paused. With a hair transplant, areas already lost can be restored using DHT-resistant donor follicles from the back and sides.
Yes. Women produce DHT in smaller amounts, but genetically sensitive follicles respond the same way. The pattern differs, typically showing as diffuse thinning across the top of the scalp rather than a receding hairline.
DHT-driven follicle miniaturization combined with inherited genetic sensitivity is the primary cause. Variations in the androgen receptor gene determine how aggressively follicles react when DHT binds to them.
DHT binds to androgen receptors in sensitive scalp follicles, shortens the growth cycle, and causes the follicle to produce thinner, shorter hair with each cycle. Over time this leads to vellus hair and then no visible growth.
Yes, if miniaturization progresses far enough for long enough. Follicles dormant for years are very difficult to reactivate without surgery. The earlier the intervention, the better the chance of partial recovery.
Not directly. But chronic stress raises cortisol, which disrupts hormone balance and can worsen pattern hair loss. Stress can also trigger telogen effluvium, a separate shedding type, which can overlap with DHT-related thinning.
It can begin in the late teens in men with strong genetic predisposition. Most commonly it becomes noticeable in the mid-to-late twenties. Earlier onset generally means more progressive loss over time.
Yes. Male pattern baldness is androgenetic alopecia. One term describes the appearance, the other describes the cause: DHT-driven follicle miniaturization in genetically susceptible individuals.
Reliable reversal through lifestyle changes alone has limited clinical evidence. Some adjustments may slow progression slightly, but they are not a substitute for finasteride or a properly assessed hair transplant.
When loss is stable, medical management is in place or being considered, and sufficient DHT-resistant donor hair exists. A hair transplant for male pattern baldness works best as part of a longer-term plan, not a standalone first step.
No. Finasteride works for most men who use it consistently, but results vary. Stage of loss and individual genetics both affect the outcome. A clinical assessment helps set realistic expectations before starting.
Years, typically. Miniaturization happens across many growth cycles. That slow pace is exactly why early changes go unnoticed, and why many people only seek help after meaningful density is already gone.
Transplanted follicles from the back and sides keep their DHT resistance in their new location permanently. But surrounding native hair that was not transplanted can keep thinning without ongoing medical management.

